


 Sign Out
Sign Out



The combination of these substances with different mechanisms of action results in increased efficacy compared to use with any of the dual component therapies. The respective mechanism of action of each drug is discussed as follows.
Budesonide, when inhaled, has a rapid (within hours) and dose dependent anti-inflammatory action in the airways, resulting in reduced symptoms and fewer COPD exacerbations. Inhaled budesonide has less severe adverse effects than systemic corticosteroids.
Glycopyrronium has a rapid onset of action and has similar affinity to the subtypes of muscarinic receptors M1 to M5. In the airways, bronchodilation is induced through inhibition of the M3 receptor at the smooth muscle.
Formoterol has a rapid onset of action. Bronchodilation is induced by causing direct relaxation of airway smooth muscle as a consequence of the increase in cyclic AMP through activation of adenylate cyclase.
As a consequence of the differential density of muscarinic receptors and β2-adrenoceptors in the central and peripheral airways of the lung, muscarinic antagonists are more effective in relaxing central airways and β2-adrenergic agonists are more effective in relaxing peripheral airways; relaxation of both central and peripheral airways with combination treatment may contribute to its beneficial effects on lung function.
Clinical efficacy and safety: The efficacy and safety of BREZTRI AEROSPHERE was evaluated in patients with moderate to very severe COPD in two randomised, double-blind, parallel-group trials.
ETHOS was a 52-week trial (N=8,588) that compared two inhalations twice daily of BREZTRI AEROSPHERE 160/7.2/5.0 micrograms or budesonide/glycopyrronium/formoterol fumarate (BGF MDI) 80/7.2/5.0 micrograms with two inhalations twice daily of glycopyrronium/formoterol fumarate dihydrate (GFF MDI) 7.2/5.0 micrograms, and budesonide/formoterol fumarate dihydrate (BFF MDI) 160/5.0 micrograms.
The primary endpoint was the rate of moderate or severe COPD exacerbations.
ETHOS was conducted in patients with moderate to very severe COPD (post-bronchodilator FEV1 ≥25% to <65% predicted) with a history of 1 or more moderate or severe COPD exacerbations in the year prior to screening. Patients were symptomatic with a COPD Assessment Test (CAT) score of 10 or above while receiving two or more inhaled maintenance therapies for at least 6 weeks prior to screening. During the screening period, the mean post-bronchodilator percent predicted FEV1 was 43%. The mean CAT score was 19.6. A total of 81% of subjects were on ICS-containing treatments prior to screening.
KRONOS was a 24-week trial (N=1,896) that compared two inhalations twice daily of BREZTRI AEROSPHERE 160/7.2/5.0 micrograms, with two inhalations twice daily of glycopyrronium and formoterol fumarate dihydrate [GFF MDI 7.2/5.0 micrograms], budesonide and formoterol fumarate dihydrate [BFF MDI 160/5.0 micrograms] and open-label active comparator Symbicort Turbuhaler 200/6 micrograms [budesonide/formoterol fumarate dihydrate]. There was a 28-week extension, for up to 52 weeks of treatment, in a subset of patients.
The two primary endpoints in KRONOS were FEV1 area under the curve from 0-4 hours (FEV1 AUC0-4) and change from baseline in morning pre-dose trough FEV1 over 24 weeks.
KRONOS was conducted in patients with moderate to very severe COPD (post-bronchodilator FEV1 ≥25% to <80% predicted), who had a CAT score of 10 or above while receiving two or more inhaled maintenance therapies for at least 6 weeks prior to screening. During the screening period, the mean post-bronchodilator percent predicted FEV1 was 50%. A prior history of exacerbations in the last 12 months was not required in KRONOS and less than 26% of patients reported a history of one or more moderate/severe exacerbations in the prior year. The mean CAT score was 18.3 and a total of 72% of subjects were on ICS-containing treatments prior to screening.
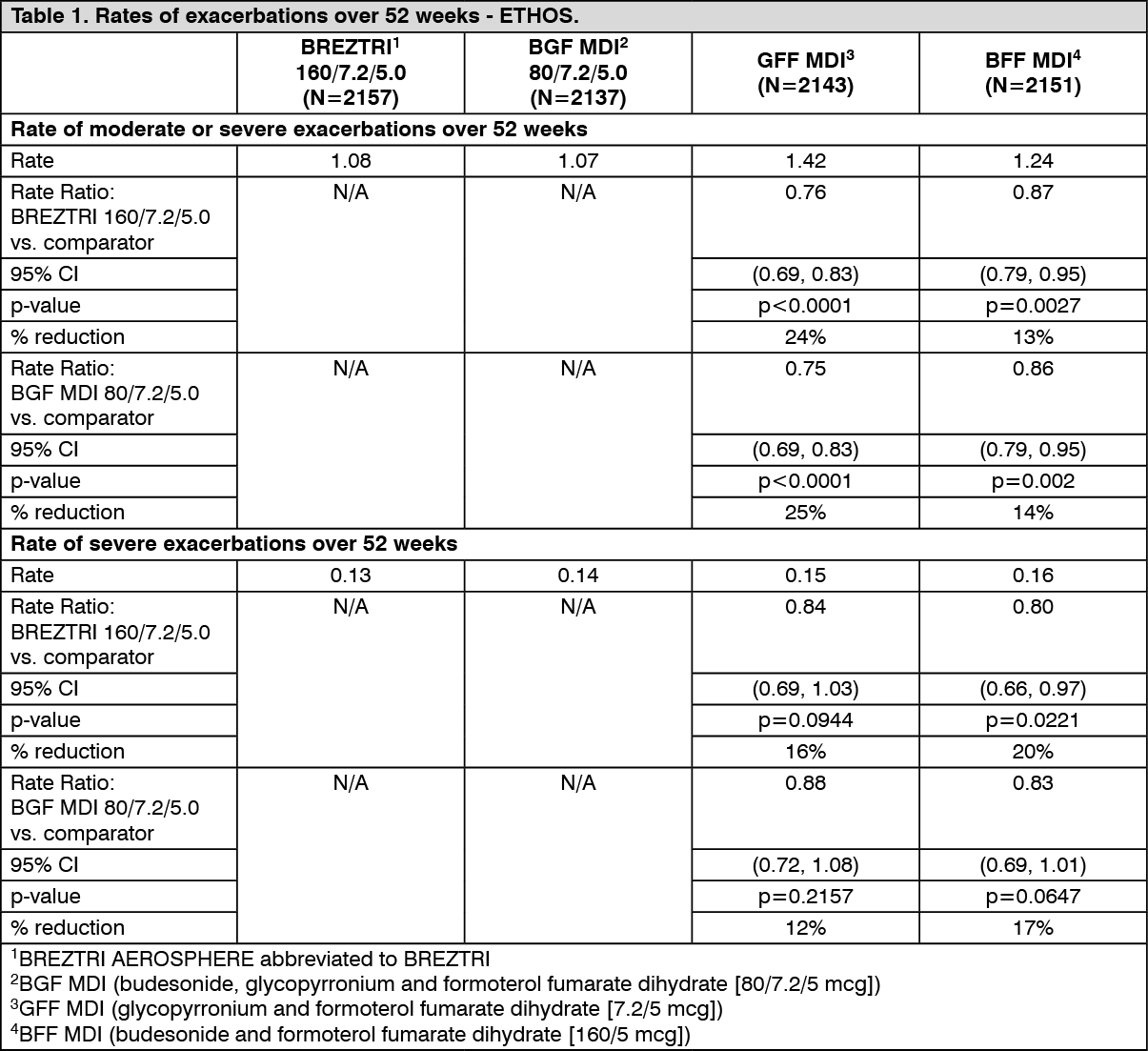
Effects on exacerbations - ETHOS: Rate of moderate or severe exacerbations: BREZTRI AEROSPHERE 160/7.2/5.0 and BGF MDI 80/7.2/5.0 significantly reduced the rate of moderate or severe COPD exacerbations over 52 weeks compared with GFF MDI and BFF MDI (see Table 1).
The benefit of BREZTRI AEROSPHERE 160/7.2/5.0 over GFF MDI in reducing the rate of moderate or severe COPD exacerbations was observed in subjects with a baseline blood eosinophil count of ≥150 cells/mm3 and those with a baseline blood eosinophil count of <150 cells/mm3. The magnitude of benefit of BREZTRI AEROSPHERE 160/7.2/5.0 over GFF MDI in reducing the rate of moderate or severe COPD exacerbations increased as blood eosinophil levels increased.
Rate of severe exacerbations: BREZTRI AEROSPHERE 160/7.2/5.0 significantly reduced the rate of severe COPD exacerbations over 52 weeks compared with BFF MDI (see Table 1).
There was a numerical reduction in the rate of severe COPD exacerbations over 52 weeks for BREZTRI AEROSPHERE 160/7.2/5.0 compared with GFF MDI, and for BGF MDI 80/7.2/5.0 compared with GFF MDI and BFF MDI (see Table 1).
Benefits on exacerbations were observed in patients with moderate, severe and very severe COPD. (See Table 1.)
 Click on icon to see table/diagram/image
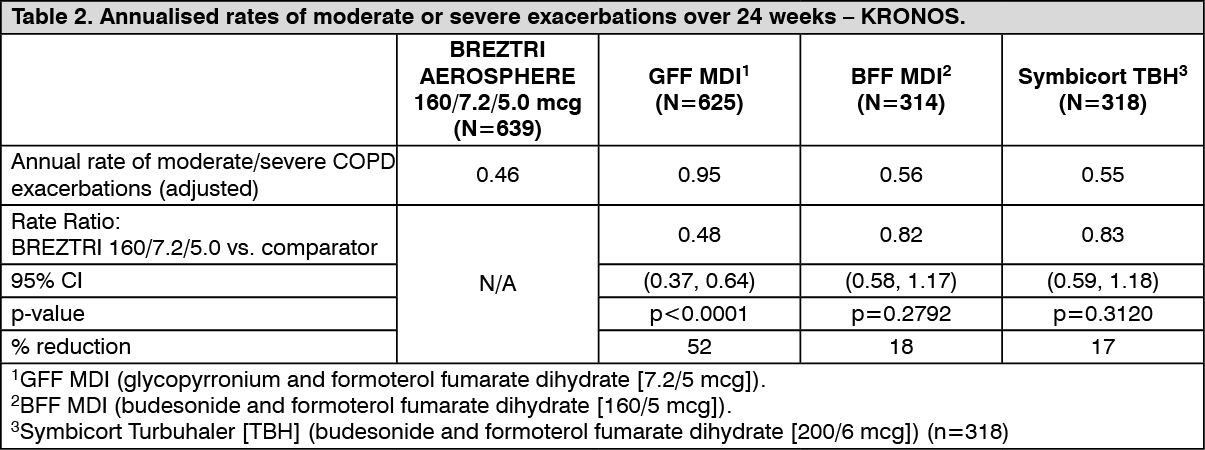
Click on icon to see table/diagram/imageEffects on exacerbations - KRONOS: BREZTRI AEROSPHERE 160/7.2/5.0 significantly reduced the rate of moderate/severe COPD exacerbations over 24 weeks compared with GFF MDI. The rate of moderate/severe COPD exacerbations was numerically lower in subjects treated with BREZTRI AEROSPHERE 160/7.2/5.0 compared to BFF MDI and Symbicort TBH (see Table 2).
In a subset of patients treated for up to 52 weeks, the effects of BREZTRI AEROSPHERE 160/7.2/5.0 on reducing moderate/severe exacerbations were generally consistent with the results up to 24 weeks.
The rate of severe exacerbations (i.e. resulting in hospitalisation or death) was significantly lower during treatment with BREZTRI AEROSPHERE 160/7.2/5.0 relative to GFF MDI (rate ratio [95% CI]: 0.36 [0.18, 0.70], unadjusted p=0.0026). The rate of severe COPD exacerbations was numerically lower in subjects treated with BREZTRI AEROSPHERE 160/7.2/5.0 compared to BFF MDI and Symbicort TBH.
Benefits on exacerbations were observed in patients with moderate, severe and very severe COPD. The benefit of BREZTRI AEROSPHERE 160/7.2/5.0 over GFF MDI in reducing the rate of moderate or severe COPD exacerbations was observed in subjects with a baseline blood eosinophil count of ≥150 cells/mm3 and those with a baseline blood eosinophil count of <150 cells/mm3. The magnitude of benefit of BREZTRI AEROSPHERE 160/7.2/5.0 over GFF MDI in reducing the rate of moderate or severe COPD exacerbations increased as blood eosinophil levels increased. (See Table 2.)
 Click on icon to see table/diagram/image
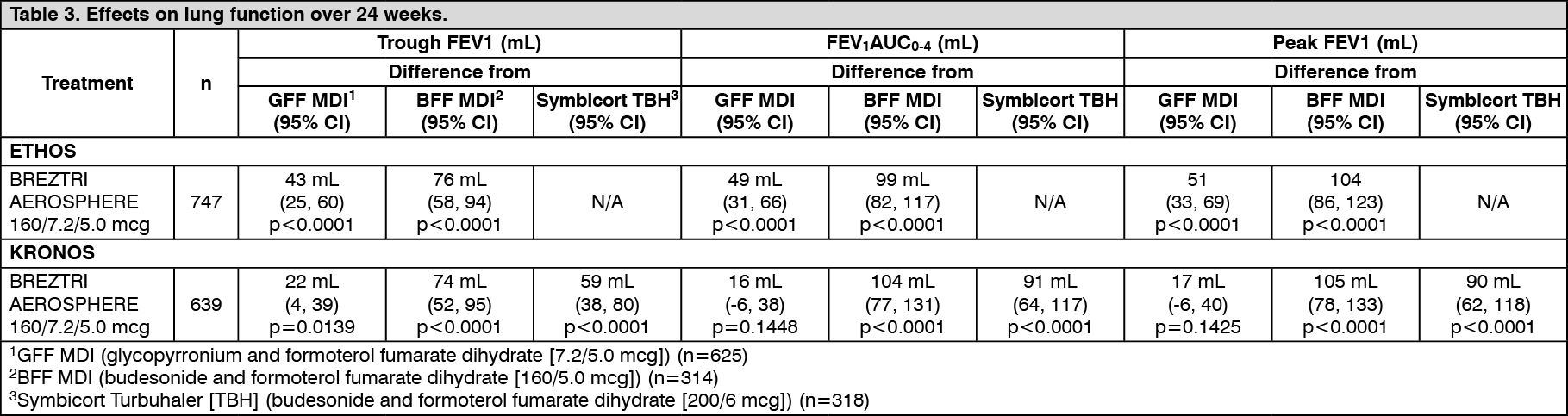
Click on icon to see table/diagram/imageEffects on lung function: In both studies, BREZTRI AEROSPHERE provided significant improvements in lung function (FEV1) compared with GFF MDI and BFF MDI (see Table 3). The improvements in lung function were sustained over 52-weeks.
The median time to a 100 mL or larger improvement was within 5 minutes of the first dose on Day 1 for all treatment groups, with a change from baseline of 166 mL (ETHOS) and 175 mL (KRONOS) for BREZTRI AEROSPHERE 160/7.2/5.0 observed at 5 minutes post-dose.
In both studies, there were consistent improvements in lung function in subgroups based on age, sex, degree of airflow limitation (moderate, severe and very severe), and previous inhaled corticosteroid use. (See Table 3.)
 Click on icon to see table/diagram/image
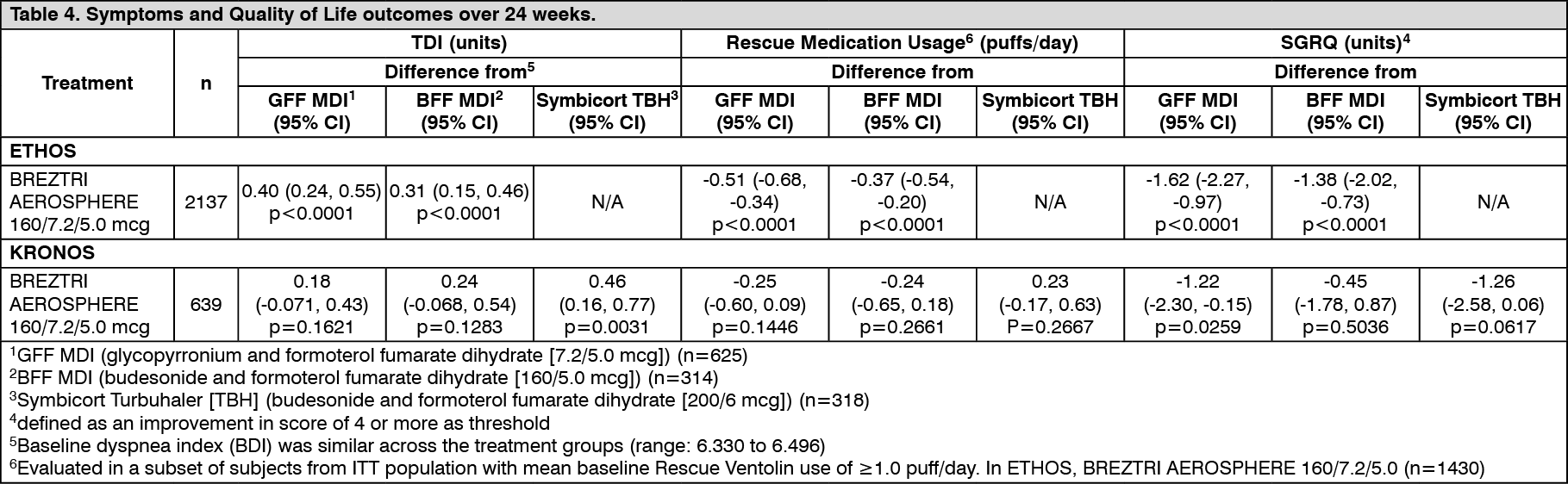
Click on icon to see table/diagram/imageEffects on symptoms and quality of life outcomes: In ETHOS, BREZTRI AEROSPHERE 160/7.2/5.0 showed significant improvements over 24 weeks in breathlessness (assessed by the Transition Dyspnoea Index [TDI]), significant reductions in the use of rescue medication and significant improvements in disease-specific health status (as assessed by the St. George's Respiratory Questionnaire [SGRQ]) compared to GFF MDI and BFF MDI (see Table 4). In patients treated for up to 52 weeks, improvements observed were generally consistent with those observed over 24 weeks.
In KRONOS, BREZTRI AEROSPHERE 160/7.2/5.0 showed numerical improvements in breathlessness (assessed by the Transition Dyspnoea Index [TDI]), numerical reductions in the use of rescue medication and numerical improvements in disease-specific health status (as assessed by the St. George's Respiratory Questionnaire [SGRQ]) compared to GFF MDI and BFF MDI (see Table 4). In patients treated for up to 52 weeks, the improvements observed were generally consistent with those observed over 24 weeks.
In ETHOS, a SGRQ responder analysis (responder defined as a reduction in SGRQ versus baseline of greater than or equal to 4) showed that there was a significantly greater percentage of responders (p<0.0001) over 24 weeks with BREZTRI AEROPSHERE 160/7.2/5 (52.2%) versus GFF MDI (42.2%) and BFF MDI (45.0%).
In KRONOS, a SGRQ responder analysis showed that there was a significantly greater percentage of responders over 24 weeks with BREZTRI AEROSPHERE 160/7.2/5.0 (47.3%) versus GFF MDI (41%; unadjusted p=0.0348), BFF MDI (39.5%; unadjusted p=0.0339) and Symbicort TBH (39.5%; unadjusted p=0.0321). (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTime to clinically important deterioration (CID): In KRONOS, the median time to a CID event was longer during treatment with BREZTRI AEROSPHERE 160/7.2/5.0 (13.5 weeks) relative to GFF MDI (12.2 weeks), BFF MDI (12.2 weeks) and Symbicort TBH (12.2 weeks).
The risk of a CID event was significantly lower during treatment with BREZTRI AEROSPHERE 160/7.2/5.0 relative to BFF MDI (HR: 0.831; unadjusted p=0.0276) and Symbicort TBH (HR: 0.811; unadjusted p=0.0119); a numerically lower risk of a CID event was observed during treatment with BREZTRI AEROSPHERE 160/7.2/5.0 relative to GFF MDI (HR: 0.877; p=0.0593).
Exacerbations of Chronic Pulmonary Disease Tool (EXACT): In ETHOS, BREZTRI AEROSPHERE 160/7.2/5.0 demonstrated a significant improvement in LS mean change from baseline in EXACT total score over 52 weeks compared with GFF MDI (LS mean difference of -1.14 units; p<0.0001) and BFF MDI (LS mean difference of -1.04 units; p<0.0001).
Evaluating Respiratory Symptoms in COPD (E-RS): In KRONOS, BREZTRI AEROSPHERE 160/7.2/5.0 demonstrated a significant improvement in LS mean change from baseline in RS Total score over 24 weeks compared with GFF MDI (-0.38; unadjusted p=0.0430); numerical improvements were observed for BREZTRI AEROSPHERE 160/7.2/5.0 compared with BFF MDI ( 0.16; p=0.4790) and Symbicort TBH (-0.16; p=0.4923).
Bone mineral density and ocular endpoints: In a subset of patients treated for up to 52 weeks in KRONOS, BREZTRI AEROSPHERE 160/7.2/5.0 was non-inferior to GFF MDI for the primary bone mineral density and ocular endpoints.
Pharmacokinetics: Lung deposition: A lung deposition study with BREZTRI AEROSPHERE 160/7.2/5.0 conducted in healthy volunteers demonstrated that on average, 38% of the nominal dose is deposited into the lung following administration with a 10 second breath-hold. The corresponding value following a 3 second breath-hold was 35%. Deposition was consistent with the width of the aerodynamic particle size distribution with both central and peripheral deposition observed.
Absorption: Budesonide: Following inhaled administration of BREZTRI AEROSPHERE in subjects with COPD, budesonide Cmax occurred within 20 to 40 minutes. Steady state is achieved after approximately 1 day of repeated dosing of BREZTRI AEROSPHERE and the extent of exposure is approximately 1.3 times higher than after the first dose.
Glycopyrronium: Following inhaled administration of BREZTRI AEROSPHERE in subjects with COPD, glycopyrronium Cmax occurred at 6 minutes. Steady state is achieved after approximately 3 days of repeated dosing of BREZTRI AEROSPHERE and the extent of exposure is approximately 1.8 times higher than after the first dose.
Formoterol: Following inhaled administration of BREZTRI AEROSPHERE in subjects with COPD, formoterol Cmax occurred within 40 to 60 minutes. Steady state is achieved after approximately 2 days of repeated dosing with BREZTRI AEROSPHERE and the extent of exposure is approximately 1.4 times higher than after the first dose.
The use of BREZTRI AEROSPHERE with the Aerochamber Plus Flow-Vu spacer in healthy volunteers increased the total systemic exposure (as measured by AUC0-t) to budesonide and glycopyrronium by 33% and 55%, respectively, while exposure to formoterol was unchanged. However, the highest increases in exposure with spacer were observed in subjects showing low exposure without spacer (most probably due to poor inhalation technique).
Distribution: Budesonide: The estimated budesonide apparent volume of distribution at steady-state is 1200 L, via population pharmacokinetic analysis. Plasma protein binding is approximately 90% for budesonide.
Glycopyrronium: The estimated glycopyrronium apparent volume of distribution at steady-state is 5500 L, via population pharmacokinetic analysis. Over the concentration range of 2-500 nmol/L, plasma protein binding of glycopyrronium ranged from 43% to 54%.
Formoterol: The estimated formoterol apparent volume of distribution at steady-state is 2400 L, via population pharmacokinetic analysis. Over the concentration range of 10-500 nmol/L, plasma protein binding of formoterol ranged from 46% to 58%.
Metabolism: Budesonide: Budesonide undergoes an extensive degree (approximately 90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6 beta-hydroxy-budesonide and 16α-hydroxy-prednisolone, is less than 1% of that of budesonide.
Glycopyrronium: Based on literature, and an in-vitro human hepatocyte study, metabolism plays a minor role in the overall elimination of glycopyrronium. CYP2D6 was found to be the predominant enzyme involved in the metabolism of glycopyrronium.
Formoterol: The primary metabolism of formoterol is by direct glucuronidation and by O-demethylation followed by conjugation to inactive metabolites. Secondary metabolic pathways include deformylation and sulfate conjugation. CYP2D6 and CYP2C have been identified as being primarily responsible for O-demethylation.
Elimination: Budesonide: Budesonide is eliminated via metabolism mainly catalysed by the enzyme CYP3A4. The metabolites of budesonide are excreted in urine as such or in conjugated form. Only negligible amounts of unchanged budesonide have been detected in the urine. The effective terminal elimination half-life of budesonide derived via population pharmacokinetic analysis was 5 hours.
Glycopyrronium: After IV administration of a 0.2 mg dose of radiolabelled glycopyrronium, 85% of the dose was recovered in urine 48 hours post dose and some of radioactivity was also recovered in bile. The effective terminal elimination half-life of glycopyrronium derived via population pharmacokinetic analysis was 15 hours.
Formoterol: The excretion of formoterol was studied in six healthy subjects following simultaneous administration of radiolabelled formoterol via the oral and IV routes. In that study, 62% of the drug-related radioactivity was excreted in the urine while 24% was eliminated in the feces. The effective terminal elimination half-life of formoterol derived via population pharmacokinetic analysis was 10 hours.
Special populations: Age, gender, race/ethnicity and weight: A population pharmacokinetic analysis of budesonide was performed based on data collected in a total of 220 subjects with COPD. The pharmacokinetics of budesonide was best described by a three-compartment disposition model with first order absorption. The typical clearance (CL/F) of budesonide was 122 L/h.
A population pharmacokinetic analysis of glycopyrronium was performed based on data collected in a total of 481 subjects with COPD. The pharmacokinetics of glycopyrronium was best described by a two-compartment disposition model with first-order absorption and linear elimination. The typical clearance (CL/F) of glycopyrronium was 166 L/h.
A population pharmacokinetic analysis of formoterol was performed based on data collected in a total of 663 subjects with COPD. The pharmacokinetics of formoterol was best described by a two-compartment disposition model with a first-order rate constant of absorption and linear elimination. The typical clearance (CL/F) of formoterol was 124 L/h.
Dose adjustments are not necessary based on the effect of age, gender or weight on the pharmacokinetic parameters of budesonide, glycopyrronium and formoterol.
There were no major differences in total systemic exposure (AUC) for all compounds among healthy Japanese, Chinese and Western subjects. Insufficient pharmacokinetic data is available for other ethnicities or races.
Elderly patients: Based on available data, no adjustment of the dosage of BREZTRI AEROSPHERE in elderly patients is necessary.
The confirmatory trials of BREZTRI AEROSPHERE for COPD included 343 subjects aged 65 and older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects.
Hepatic impairment: No pharmacokinetic studies have been performed with BREZTRI AEROSPHERE in patients with hepatic impairment. However, because both budesonide and formoterol are primarily eliminated via hepatic metabolism, an increased exposure can be expected in patients with severe liver impairment. Glycopyrronium is primarily cleared from the systemic circulation by renal excretion and hepatic impairment would therefore not be expected to effect systemic exposure.
Renal impairment: Studies evaluating the effect of renal impairment on the pharmacokinetics of budesonide, glycopyrronium and formoterol were not conducted.
The effect of renal impairment on the exposure to budesonide, glycopyrronium and formoterol for up to 24 weeks was evaluated in a population pharmacokinetic analysis. Estimated glomerular filtration rate (eGFR) varied from 31-192 mL/min representing a range of moderate to no renal impairment. Simulation of the systemic exposure (AUC0-12) in subjects with COPD with moderate renal impairment (eGFR of 45 mL/min) indicates an approximate 68% increase for glycopyrronium compared to subjects with COPD with normal renal function (eGFR of >90 mL/min). Renal function was found not to affect exposure to budesonide or formoterol.
Toxicology: Preclinical safety data: Non-clinical data reveal no specific hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and carcinogenic potential.
The toxicity observed in animal studies with budesonide, glycopyrronium and formoterol was similar, whether they were given in combination or separately. The effects were associated with pharmacological actions or minor adaptive responses commonly observed in inhalation toxicology studies and dose dependent.
No genotoxicity, carcinogenicity or reproductive toxicology studies have been conducted with BREZTRI AEROSPHERE.
In animal reproduction studies, glucocorticosteroids such as budesonide have been shown to induce malformations (cleft palate, skeletal malformations). However, these animal experimental results are not relevant in humans at the recommended doses (see Use in Pregnancy & Lactation). Budesonide demonstrated no tumourigenic potential in mice. In rats, an increased incidence of hepatocellular tumours was observed, considered to be a class-effect in rats from long-term exposure to corticosteroids.
Animal reproduction studies with formoterol have shown a slightly reduced fertility in male rats at high systemic exposure and implantation losses, as well as decreased early postnatal survival and birth weight at considerably higher systemic exposures than those reached during clinical use. A slight increase in the incidence of uterine leiomyomas has been observed in rats and mice treated with formoterol; an effect which is considered to be a class-effect in rodents after long-term exposure to high doses of β2-adrenoreceptor agonists.
Animal reproduction studies with glycopyrronium have shown reduced rat and rabbit foetal weights, and low body weight gain of rat offspring before weaning, only at very high doses compared to clinical use. No evidence of carcinogenicity was seen in 2-year studies in rats and mice.
BREZTRI AEROSPHERE contains the excipients 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC) and calcium chloride as part of the spray-dried porous particle technology in the pressurised liquid propellant HFA-134a. The safety of HFA-134a has been fully evaluated in preclinical studies. DSPC and calcium chloride have a long history of safe use in man and are approved excipients worldwide. Furthermore, inhaled toxicology studies carried out with BREZTRI AEROSPHERE have shown no evidence of any toxicity attributable to the excipients.